Procurement is a pillar of a well-functioning health system, ensuring timely and reliable access to medicines, vaccines, and health products. Yet in many countries, procurement systems remain weak, offering limited skills and expertise and few sustained efforts to strengthen country-level institutions. Although global and supranational methods for acquiring goods and services have helped shape markets and ensure supply at scale, they also inadvertently reduced global donors' willingness to invest in robust national procurement systems.
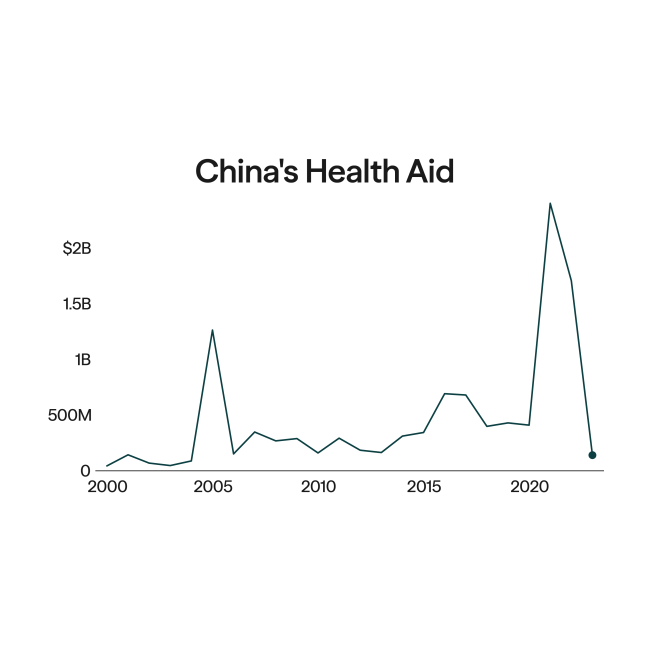
Now, the discussion around the locus of procurement—the "where and how"—has become more consequential considering the United States' shift toward financing global health through government-to-government (G2G) memoranda of understanding. The United States spends roughly $1.3 billion annually on commodity procurement for HIV, TB, malaria, and polio, a sizable component of U.S. global health spending.
Two different directions could be taken. On one hand, under the America First Global Health Strategy and G2G memoranda, procurement responsibility could shift more directly to recipient governments.
On the other hand are discussions about expansion by creating or strengthening pooled procurement, such as the Global Fund's centralized model; examples run by regional bodies such as the African Pooled Procurement Mechanism (APPM); or private platforms such as Axmed and Proqurable. Although global pooled procurement can lower prices, studies suggest that more aggregated procurement is associated with price reductions of roughly 15–20%, but these effects vary significantly by market structure and country characteristics.
15–20%
More aggregated procurement is associated with roughly 15–20% price reductions
Policy debates around procurement pooling and aggregation, when multiple buyers combine demand or coordinate purchasing to secure lower prices and more stable supply, often lack sufficient nuance. The operational questions are more specific: For which products, in which markets, and for which countries do pooled or aggregated procurement add value relative to other modalities such as national, regional, or private procurement platforms? Does pooling procurement above the country level impose trade-offs in lead time, flexibility, local manufacturing preferences, financing constraints, or risk appetite? Could a multilane procurement architecture, a system under which countries choose among multiple procurement channels, still support healthy global market dynamics?
Three reasons explain why these questions matter for the America First Global Health Strategy. If donors treat a single platform as the primary solution for procurement aggregation, several predictable problems can arise. First, mismatched constraints, such as pre-payment requirements or regulatory conditions incompatible with national procurement laws or financing systems, are possible. Performance trade-offs could be presented as improvements when gains in transparency or reliability require earlier ordering and reduced flexibility. And, by making one procurement channel the default, it could crowd out national and regional innovation.
Instead, donors can focus on building an information architecture that allows procurement lane choices to be transparent and performance-based through systematic third-party benchmarking of procurement systems. Rather than a one-time assessment, benchmarking should operate as a dynamic information platform allowing continuous comparison across procurement models. Such a system could incorporate tiered access levels, enabling insights to be shared without requiring full public disclosure of prices or contractual terms.

For many routine medicines—particularly generics with multiple suppliers—countries of reasonable size can achieve meaningful bargaining leverage without cross-border pooling if they organize and govern their procurement systems well. However, research highlights that international pooling is most effective for small buyers and highly concentrated markets, such as new health technologies or medical countermeasures.
This points to the fact that the real opportunity may go beyond simple pooling and further toward more standardized product specifications, streamlined regulatory pathways, and incentives for manufacturers to register products across markets that can improve competition and supply reliability without requiring all procurement to be centralized globally.
Pooled Platforms Are Not Universally Appropriate
Besides the price benefits, an additional benefit of pooled procurement is that it can improve reliability and reduce delivery delays, but the mechanism is often misunderstood [PDF].
Global pooled platforms typically rely on long-term supplier agreements combined with forward demand forecasts. Suppliers commit to tighter delivery timelines once orders are placed. Research has found that when the share of orders routed through the Global Fund's Pooled Procurement Mechanism increases from 0% to 100%, the share of delayed orders falls by 26%, suggesting improved delivery reliability. Similar results have been seen with procurement structures that were used by the U.S. Agency for International Development (USAID) programs such as the President's Emergency Program for AIDS Relief (PEPFAR) and the President's Malaria Initiative.
$1.7 billion
More than $1.7 billion is spent on essential commodities annually through the Global Fund's Wambo platform
However, this reliability improvement comes with a trade-off. Pooled procurement often requires earlier ordering and financial commitments from buyers. One perspective is that this forces better planning discipline at the country level; others say it reduces flexibility, especially when demand is uncertain or conditions change.
This tension is why pooled procurement is not a one-size-fits-all solution. When countries prioritize speed, flexibility, or responsiveness, pooled procurement may be less attractive even if headline prices are lower.
As an example, the Global Fund's Wambo platform, which oversees the Fund's pooled procurement mechanism, has become a major channel. More than $1.7 billion is spent on essential commodities annually [PDF] through it, involving more than 2,000 purchase orders and nearly 5,000 shipments. The mechanism contributes to better prices and provides market certainty for medicine suppliers.
However, questions remain about whether the platform has consistently reduced lead times, a 2017 Office of the Inspector General report [PDF] finding that it did not achieve a target of 21- to 26-day order processing times. Another benefit of the Wambo platform results from how it increases suppliers' confidence about early and timely payment, as well as making the operational steps in procurement processes more efficient. However, these benefits don't always apply when countries use their own funds to purchase through Wambo.
The point is not that this platform lacks value. Instead, its value is not synonymous with universal appropriateness, nor is it necessarily suitable as the dominant procurement channel for bilateral donor programs.
Where Pooled Procurement Is Valuable
Pooling can add the greatest value for medical countermeasures and newly introduced technologies. These markets often have limited suppliers, uncertain demand, constrained manufacturing capacity, regulatory complexity, and high-fixed costs for entry.
In these settings, pooled procurement can support earlier market entry through credible aggregated demand and advanced commitments, standardized quality requirements and eligibility rules, and coordinated allocation when supply is scarce that can reduce panic buying.

However, global pooled procurement cannot assume uniform national preferences, as shown by the experience with the COVID-19 vaccine. Countries differ in risk tolerance, speed preferences, financing constraints, and political priorities. Some may accept higher prices or regulatory risk to access new technologies earlier. Others prioritize lower prices, stronger quality assurance, or coordinated allocation mechanisms. Both strategies are rational. Problems arise when procurement architecture removes these choices or when decisions occur without transparency or coordination.
A workable system should therefore assume that multiple procurement channels will coexist, countries choosing among modalities based on their preferences, perceived benefits, and sovereignty considerations.
Multilane Procurement
Multilane procurement depends on preferences around price, reliability, lead time, local manufacturing objectives, and risk appetite.
In practice, countries already purchase health products through a mix of
- national procurement, typically through central medical stores or national tenders;
- global pooled mechanisms, often tied to donor financing and quality assurance requirements;
- upcoming regional platforms, often linked to industrial policy and manufacturing objectives; and
- new and upcoming private procurement marketplaces, which include financing mechanisms and supplier analytics.
Procurement systems in Africa and other low- to middle-income countries (LMICs) are already multilane and will likely become more so. Yet the very mention of multilane procurement raises concerns among global stakeholders. Critics worry that it could increase transaction costs, discourage global manufacturers from serving these markets, weaken market-shaping efforts, and compromise quality.
Many of these concerns are valid. In fragile markets such as those for low-volume products, pediatric formulations, early-phase technologies, and medical countermeasures with limited supply, poorly coordinated multilane procurement could create real challenges because fragmented signals about demand don't allow manufacturers to plan associated production. It could also reduce the ability to negotiate single long-term price and delivery agreements. Quality standards not harmonized across procurement pathways also create risks of poor quality and diffuse accountability for quality. But the central question is different: If multilane procurement reflects country preferences and political economy realities, can systems be designed to manage the associated downsides? This would require coordination of market information, demand signals, contract performance data, quality assurance, and exception management.
There are precedents for such coordination. For example, the Antiretroviral Procurement Working Group (APWG) helped stabilize pediatric HIV markets by sharing information, synchronizing procurement cycles, and coordinating purchasing strategies across national and global procurers. Similarly, the Global Family Planning Visibility and Analytics Network (VAN) links procurers, manufacturers, and countries through shared data governance to align demand forecasting, production planning, procurement, and funding flows. These examples may not be ready for the scale that multilane procurement across medicines might require, but they do illustrate that multiple procurement channels can coexist when supported by information sharing and light coordination mechanisms.
National Procurement Has Pockets of Excellence
A common narrative is that national procurement capacity is weak. Governance and technical challenges exist, but so do notable examples of innovation.
Rwanda Medical Supply not only procures a range of products at competitive prices, but has also executed a reverse auction for specific medical products that leads to real-time price discovery and helps secure better prices quickly. Even large global health procurement agencies—despite their scale and market influence—have rarely adopted mechanisms such as reverse auctions in their procurement models. Such innovations demonstrate that national procurement systems can develop sophisticated approaches when incentives and capacity are aligned. The Global Fund, the U.S. government, and the World Bank should direct grant funding toward building national procurement systems like the ones that have emerged as pockets of excellence.
Regional Procurement and Private Procurement Marketplaces
Regional procurement efforts are also expanding. The APPM led by the Africa Centres for Disease Control and Prevention aims to aggregate demand across the continent to strengthen bargaining power, stabilize supply, and support regional manufacturing. Regional blocs such as the Southern African Development Community, the East African Community, and Small Island Developing States are exploring joint procurement arrangements for essential medicines.
At the national level, Nigeria has launched MediPool, a group purchasing organization designed to aggregate demand across public and private health facilities.
Concurrently, private procurement marketplaces are emerging that combine procurement execution with supplier analytics, prequalification systems, and potential financing solutions. Platforms such as Axmed and Proqurable provide procurement services to private wholesalers and government purchasers on an opt-in basis for when their value proposition aligns with buyer needs. Which of these efforts will succeed at scale remains uncertain. But that is precisely why a multilane procurement approach is a no-regrets strategy—allowing progress across multiple pathways while new institutional models evolve.
Multilane procurement is not a sign of dysfunction or fragmentation. It reflects how health systems are financed, governed, and politically negotiated. The real policy challenge is therefore not to substitute multilane procurement with a single pooled procurement structure, but instead to design systems that coordinate it effectively using shared information, transparency, and performance rules.