In late February 2025, the United States canceled two aid programs in Cambodia: one to promote child literacy, the other to improve nutrition for children younger than 5. The price tag was $40 million—a modest sum in Washington's ledger, but substantial for a country whose entire gross domestic product (GDP) is comparable to Vermont's.
A week after the cancellation, China's aid agency announced funding for projects with near-identical aims. "Children are the future of the country and the nation," Wang Wenbin, China's ambassador to Cambodia declared, standing alongside the Southeast Asian country's health minister. "We should care for their healthy growth together." The sequence was striking. The optics were choreographed.
In a region marked by persistent gaps in health-system capacity and access to care, Chinese assistance is necessary and consequential. This support has expanded access and delivered tangible benefits through Southeast Asia's infrastructure, supply chains, and institutional partnerships. This contribution grows more significant as the United States scales back its global health commitments.
Yet the architecture surrounding this engagement is reconfiguring relationships in subtle ways that may prove enduring, amounting to an emerging architecture of dependency. The question, then, is not whether China's role is welcome but what kind of regional health order it is quietly building, and at what cost to Southeast Asia's long-term autonomy.
A Region of Unmet Needs
The health-care landscape in Southeast Asia is characterized by stark and persistent inequality. Whereas Singapore boasts a world-class health system and Thailand has achieved near-universal coverage, countries such as Cambodia, Laos, and Myanmar continue to struggle with basic service delivery, particularly in rural and hard-to-reach areas where infrastructure, equipment, and trained personnel remain scarce.
Across the region, unmet health-care needs remain persistent and complex. The Mekong subregion continues to be a global hotspot for drug-resistant malaria, and the Philippines grapples with one of the world's fastest-growing HIV epidemics and a heavy burden of drug-resistant tuberculosis. These epidemiological challenges are compounded by protracted conflict: insurgencies in Indonesia, the Philippines, and Thailand, along with Myanmar's ongoing civil war, have placed additional strain on fragile health systems.
For lower-income members of the Association of Southeast Asian Nations, external health intervention is less a voluntary option than a structural necessity
Over the past decade, international partners—most notably the United States—have played a central role in financing and delivering public health interventions. Between 2018 and 2023, the President's Malaria Initiative (PMI) channeled approximately $100 million to support programs across Cambodia, Laos, Myanmar, and Thailand, funding insecticide-treated mosquito nets, rapid diagnostic tests, and frontline antimalarial treatments. Meanwhile, the President's Emergency Plan for AIDS Relief (PEPFAR) has invested nearly $1 billion in Vietnam since 2004, expanding HIV testing and antiretroviral therapy, and it was extended to the Philippines in 2022 to strengthen prevention and treatment efforts. Along the Myanmar-Thailand border, U.S. aid has underwritten a fragile but essential health infrastructure for displaced communities, supporting NGO-run clinics, maternal and child health services, vaccination, and referrals through partners such as the International Rescue Committee.
For lower-income members of the Association of Southeast Asian Nations (ASEAN), external health intervention is less a voluntary option than a structural necessity. Domestic financing and health-system capacity are struggling to keep pace with the scale of health-care demand: ASEAN is home to 684 million people, and its older population is projected to more than double by 2050, reaching 22% of the population, accelerating demand for chronic-disease, geriatric, and palliative-care services. The region faces a growing burden [PDF] of noncommunicable diseases even as many member states continue to face workforce shortages, high out-of-pocket spending, and uneven access to primary care.
A 2022 systematic review of health financing in Southeast Asia identified limited government spending, fragmented risk pooling, a large informal health workforce not covered by social health insurance schemes, and rising health-care costs as persistent structural weaknesses that make health systems vulnerable to donor influence. The same review found that government health allocations fell below 9% of total budgets in Indonesia, Laos, Malaysia, the Philippines, and Vietnam. In Laos and Cambodia, external donors provided 14.5% and 16.4% of total health expenditure respectively—a level of dependence that raises serious questions about sustainability and sovereign control over health priorities, since recipient governments hold little authority over how funds are directed.
What Has Been Cut, and What It Means
External funding does not merely fill gaps; it reshapes the boundaries of domestic health planning when governments lack control over the source, duration, and priorities of financing. Donor-funded programs may not align with national health needs, resulting in public health projects defined by external priorities rather than local ones. Many recipient countries also rely on short-term earmarked funding for health rather than receiving sustained institution- and capacity-building. Southeast Asia is now entering a period of sharply shrinking development finance. According to a 2025 report by the Lowy Institute, official development finance to the region could fall by more than $2 billion by 2026, as bilateral aid is expected to decline by around 20%—from $11.3 billion in 2023 to $9 billion in 2026.
The consequences of the U.S. retreat from global health are already rippling across Southeast Asia. Under the second Trump administration, the withdrawal of funding and operational support has left significant gaps in programs long dependent on U.S. backing. As recently as last year, the U.S. Agency for International Development (USAID) allocated approximately $860 million to Southeast Asia, with health among its core priorities, spanning six countries: Cambodia, Laos, Myanmar, the Philippines, Thailand, and Vietnam.
The distribution of this assistance was uneven, and so too is the impact of its withdrawal. Cambodia, Indonesia, Myanmar, the Philippines, and Vietnam were among the largest recipients. Yet Cambodia and Myanmar stand to suffer most because aid constituted a large share of their economies, and their health, governance, and humanitarian sectors will bear the heaviest burden of cuts.

In the Mekong subregion, the rollback of U.S. funding risks reversing decades of progress in malaria control, placing millions at renewed risk. In Vietnam, the reduced support has disrupted 92 PEPFAR-funded facilities, on which 70% of patients rely for HIV services. The situation is similar in the Philippines. Along the Myanmar-Thailand border, clinics serving displaced populations have closed or consolidated amid funding shortfalls, contributing to the first confirmed deaths linked to the aid freeze. Estimates from the Center for Economic and Policy Research suggest that USAID program suspensions could result in 500,000 to 700,000 additional deaths annually.
Into this widening gap, new providers have stepped forward. China has moved decisively, positioning itself as a partner in crisis and steward of global health governance—with ambitions not merely to deliver assistance but to shape the terms on which it is given.
What China Provides and How
The financial backdrop sharpens the stakes. Official development finance to Southeast Asia reached $29 billion in 2023, up from $26.5 billion in 2022, but still below the prepandemic average of $33 billion. The rebound was driven mainly by nonconcessional loans from China, the Asian Development Bank, and the World Bank, rather than by grants or concessional health and social spending. In the wake of major Western aid cuts, the region's development-finance center of gravity is shifting increasingly to Beijing. The region's need for Chinese health assistance should therefore be understood against this structural backdrop. Many states are not choosing between autonomy and aid but between unmet health needs and externally financed provision.
Although China's increased prominence in Southeast Asia's health landscape appears new, the underlying playbook is well rehearsed. The COVID-19 pandemic served as an accelerant and a template: in 2020, as global supply chains fractured and Western countries turned inward, Beijing moved quickly to supply masks, testing kits, and, later, vaccines to countries such as Cambodia, Laos, and Myanmar, in what became known as mask and vaccine diplomacy. These early deliveries were highly visible, often accompanied by official ceremonies and framed not only as emergency relief but as gestures of solidarity. The same playbook is now being reprised in the wake of U.S. withdrawal from health aid: rapid provision, clear attribution, and tightly managed bilateral delivery.
Beyond emergency response, China's health-care contributions are anchored in physical infrastructure, a familiar feature of its engagement across the Global South. Hospitals constructed with Chinese financing are frequently framed as symbols of bilateral friendship, infusing political meaning into clinical spaces. The Cambodia-China Friendship Preah Kossamak Hospital is emblematic: a modern facility built in Phnom Penh by Chinese contractors and equipped through Chinese procurement channels. Yet such projects are not merely buildings. They embed a wider technical ecosystem—medical equipment, supply chains, maintenance protocols, contractor warranties, and after-sales servicing—that ties recipient countries to Chinese vendors and expertise long after construction is completed. Infrastructure arrangements create structural dependencies not only through debt or financing but through the everyday requirements of keeping clinical systems operational.
Alongside bricks and mortar, Beijing is weaving together human linkages. Rotating Chinese medical teams have been dispatched to underserved settings across the region, providing clinical care while reinforcing state-to-state ties. Scholarships and training exchanges bring Southeast Asian medical students and professionals to China through initiatives like the China-ASEAN University Alliance for Medicine and the China-ASEAN Community of Medicine and Health, cultivating a cohort of regional health professionals whose training, networks, and institutional affiliations are grounded, in part, in Chinese frameworks.
No external actor in the region can match Beijing's financial capacity, speed of delivery, scale of resources, or tolerance for political risk
These engagements are being formalized. The inaugural China-ASEAN Public Health Cooperation Forum in 2023, alongside discussions of a cross-border health corridor along Yunnan's borders, points toward structured mechanisms for data sharing, emergency response, and routine collaboration. Over time, these people-to-people exchanges deepen familiarity and alignment in ways that outlast any single project cycle.
No external actor in the region can match Beijing's financial capacity, speed of delivery, scale of resources, or tolerance for political risk. Chinese provision has, in many cases, filled real gaps. Hospitals built with Chinese financing are functioning institutions treating patients in settings where alternatives were absent, and educational partnerships have equipped local clinicians with skills carried back into domestic health systems, producing measurable, if uneven, improvements in service delivery. Because it addresses genuine need, this assistance is welcomed rather than merely tolerated, and this legitimacy is partly what makes the structural dependencies it creates so difficult to unwind.
The Architecture of Dependency
At the seventy-second World Health Assembly in 2019, the head of China's National Health Commission declared that the country would "join hands with relevant nations to address health challenges" and make "positive contributions to seeking the health and well-being of all human beings." These initiatives are increasingly subsumed under the Health Silk Road, a health-focused arm of the Belt and Road Initiative (BRI) launched in 2015. China has leveraged BRI-built transportation networks—railways, ports, airports, and logistics hubs—to deliver [PDF] medical supplies and services, positioning itself not only as a provider of aid but as a coordinator of regional health flows.
The framing is deliberate. By embedding health assistance within a wider architecture of infrastructure, trade, and geopolitical integration, Beijing makes it increasingly difficult to disaggregate Chinese hospitals, medical supply chains, and training programs from its broader regional strategy. The ambition, in other words, is not to intervene but to integrate.
The architecture of that system is as significant as the volume of aid delivered. China's health investments in Southeast Asia are neither ad hoc nor opportunistic; they serve a defined set of geopolitical objectives, providing health care to ASEAN states on terms that reflect Beijing's strategic priorities. After the severe acute respiratory syndrome (SARS) pandemic in 2003, China formally reframed public health as a nontraditional security concern—one tied to border stability, regional image, and economic continuity—and Southeast Asia became the central theater for that reorientation. What followed was not a scatter of one-off donations but a layered architecture of disease surveillance, clinical training, medical supply chains, and institutionalized cooperation mechanisms embedded within China's regional frameworks.
The forms this architecture takes are concrete. In the Mekong region, China has constructed a disease-control infrastructure spanning borders that includes malaria service stations, joint surveillance workstations, diagnostic laboratories, and community volunteer networks across Cambodia, Laos, Myanmar, and Vietnam. Between 2011 and 2024, health organizations in China's Yunnan province alone trained more than 10,000 public health personnel from mainland Southeast Asian countries and dispatched more than 100 expert teams.

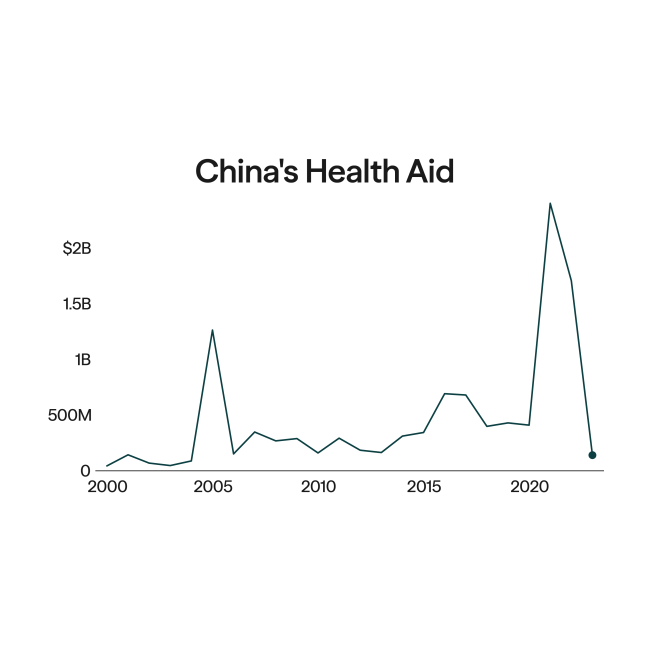
The COVID-19 pandemic laid bare the strategic logic of this architecture. Southeast Asia emerged as a priority region for China's mask and vaccine diplomacy, largely because of its central importance to Beijing's Belt and Road Initiative as the preferred corridor for the Twenty-First Century Maritime Silk Road. China repurposed its Belt and Road logistics networks into vaccine delivery channels, directing 44% of its roughly 1.6 billion committed doses to the region by October 2021—the same area that hosted the heaviest concentration of Belt and Road construction. Vaccine diplomacy and geopolitical integration followed the same map. The same logic explains the shifting regional priorities of China's overall health aid. During 2005–13, 4 of the top 5 recipients of Chinese development assistance for health were African nations. By the 2020–21 period, however, Southeast Asia had become the clear priority, as Cambodia, Laos, Myanmar, and the Philippines all ranked among the largest recipients worldwide.
The implementation logic is consistently bilateral and state-to-state. Agreements are brokered between governments rather than routed through multilateral intermediaries. Civil society and local communities are seldom consulted in design or delivery. China has progressively incorporated cross-border disease prevention into the Belt and Road Initiative and the Lancang-Mekong Cooperation framework, binding health cooperation to the same bilateral architecture that governs infrastructure and trade. Visibility remains integral. Projects are branded, ceremonies are staged, and Beijing takes credit in national media on both sides. The result is a model in which gratitude compounds between states, and where the deepening of health ties quietly deepens the broader relationship on China's terms.
… disentanglement would mean dismantling systems that recipient countries have come to rely on
Yet evidence on China's development assistance for health complicates a purely strategic reading of Chinese health aid. Across 82 recipient countries, a 2018 analysis found that allocation is more strongly associated with recipient need and merit than with donor interests such as trade or natural-resource access. GDP per capita was a significant predictor of overall allocation, while health workforce shortages and malaria burden were associated with specific aid modalities such as medical teams and antimalaria centers. China's engagement, in other words, is not simply predatory; it responds to real gaps, which makes the structural dependencies it creates more nuanced and difficult to contest.
What makes China's assistance durable, therefore, is not coercion but the absence of any single point of pressure. China does not condition health aid explicitly, nor does it pull back funding when political alignment falters, relying instead on softer mechanisms: market dependence, supply-chain integration, and institutional lock-in. Dependencies accumulate through the routine functioning of health systems rather than through moments of pressure.
Once Chinese surveillance platforms, training pipelines, procurement channels, and technical standards become part of routine health governance, the cost to exit rises with each passing year—not because Beijing demands it but because disentanglement would mean dismantling systems that recipient countries have come to rely on. This path-dependent lock-in is the architecture's quiet logic: influence operates through alliances rather than ultimatums, and alignment emerges from accumulated inertia rather than compulsion. An architecture that shapes behavior without ever needing to announce itself is, for that reason, the hardest to contest.
Regional Architecture for Greater Autonomy
China is shaping Southeast Asia's regional health order in ways that are predominantly bilateral and dependency-reinforcing, limiting recipient governments' room for political maneuver and their ability to exert independent control over their health systems. If Southeast Asia is to assert greater autonomy over its own health governance, the response is not to wait for a more magnanimous patron. Instead, it requires more committed action to accelerate what regional health collaboration has long promised but underdelivered.
ASEAN already possesses the levers it could activate more forcefully by capitalizing on existing institutional mechanisms. First, it could expand its financing role. The ASEAN Infrastructure Fund could channel more capital into health infrastructure, offering concessional terms to lower-income members and reducing reliance on single-country supply chains for hospital construction.
Second, ASEAN could invest more systematically in its own human capital. A regional mentorship program pairing high-performing health systems such as Singapore and Thailand with lower-capacity members could strengthen clinical training, hospital management, and health governance, raising overall standards.
Third, the region could play a more active role in shaping investment flows by establishing a health-investment facilitation framework and diversifying health financing beyond state-led bilateral models. ASEAN could more actively court nontraditional financiers: private philanthropies, corporate actors, and multilateral development funds that have already demonstrated a footprint in the region.
Wellcome Trust has embedded research infrastructure across the Mekong through the Mahidol Oxford Tropical Medicine Research Unit in Thailand and the Oxford University Clinical Research Unit in Vietnam, both of which strengthen local scientific capacity rather than substituting for it. Takeda Pharmaceutical has run multiyear maternal and newborn health programs across Laos, Myanmar, and Vietnam in partnership with Save the Children, and it supports nutrition supply chains in Indonesia. The Islamic Development Bank has provided $1.4 billion in financing for health projects in Indonesia alone, adding more than a thousand hospital beds across six facilities. A coordinated ASEAN framework for engaging these actors, rather than leaving each member state to negotiate bilaterally, could pool leverage, set common standards, and direct capital toward shared regional priorities.
These frameworks and initiatives will take time to mature and are not intended to displace China's role in the region, nor should they be. Chinese health-care assistance has met real needs, expanded access in underserved areas, and delivered tangible benefits to recipient countries; its presence in Southeast Asia has been durable and, in many respects, welcome. The challenge confronting the region is not whether to accept China's health-care assistance but how to do so without foreclosing alternatives and entrenching dependency.
ASEAN has embedded structural constraints: persistent development disparities among member states, the absence of supranational authority and enforcement mechanisms, and the "ASEAN way" of consensus and non-interference all impede effective decision-making on urgent issues. If ASEAN is to shape, rather than simply receive, the terms of external health-care engagement, it must invest more heavily in regional health cooperation and designate health care as a political priority.
Strengthening institutional capacity is a governance opportunity ASEAN can no longer defer.