In April 2026, the State Department released key results data from 2025 for programs supported by the U.S. President's Emergency Plan for AIDS Relief (PEPFAR). Although the release provided some insight into the performance of the U.S. HIV programs, data on the rest of the global health portfolio remains inaccessible to the public.
Soon after the Trump administration began dismantling the U.S. Agency for International Development (USAID) in January 2025, the public archive documenting the program's achievements was taken down. Working with limited information, researchers are still trying to quantify the short- and long-term health effects of shifts in foreign aid, including changes in preventable deaths and disease burden. A February 2026 Lancet analysis estimates that continued funding cuts could result in more than 14 million additional deaths by 2030, including about 4.5 million children younger than 5.
Modeled estimates tell part of the story, but actual data on U.S.-funded global health achievements will be critical to understanding what has happened to health on the ground and how the cuts could be felt in years to come. Without public access to the historical baseline data for these same indicators, it is impossible to assess whether proposed targets reflect realistic continuation of past trends, account for transition-related disruptions, or align with what is needed to maintain progress toward global health goals—particularly as U.S. strategy shifts away from aid and toward bilateral health deals with recipient governments.
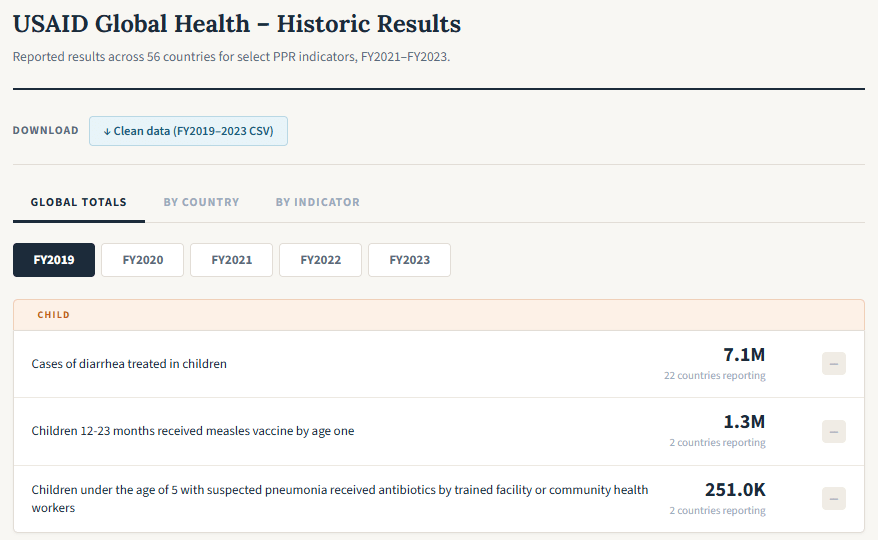
Building on efforts to preserve U.S. government data across sectors before they disappear, former USAID officials built a new interactive tool that recovers USAID global health data from the Wayback Machine, an internet archiving site, to preserve available results for the public. The tool displays available USAID global health data from fiscal years 2019 to 2023 across countries, health areas, and select indicators, providing a record of past achievement, accompanied by a downloadable dataset.
A Disappearing Record
For more than a decade, the U.S. Performance Plan and Report (PPR) system served as the definitive source of performance-monitoring data across government global health programs, tracking service delivery in maternal and child health, malaria, tuberculosis (TB), nutrition, and family planning, as well as work supporting health systems strengthening and global health security annually. The State Department reported HIV program data separately and made it publicly available through dedicated PEPFAR reporting channels. Collectively, these standardized, annual reporting processes provided the official historical record of U.S. global health results, which Congress used to inform decisions on where to appropriate global health funds. Partner governments and other donors relied on the data to coordinate investments and avoid duplication. Researchers and civil society used it to hold the government accountable for delivering on global health goals.
Historically, USAID released PPR data annually through the Dollars to Results platform. The website has been dark since early 2025, and, with it, a substantial record of achievement has been erased. The new tool shows that in 2023, the last year of available data, USAID purchased nearly 50 million insecticide-treated bed nets in fiscal year 2023, helped 12 million women deliver their babies in health facilities, and reached 28.2 million children younger than 5 with nutrition interventions.
Data from fiscal year 2024, which was being finalized when the USAID's awards were terminated and staff placed on administrative leave in early 2025, remains unreleased. It is unclear whether the State Department proceeded with data collection in fiscal year 2025 as planned, and whether it will release the data publicly if available.
Measurement Matters
The incomplete public record of U.S. global health performance has implications beyond the erasure of USAID's past achievements.
The State Department's America First Global Health Strategy emphasizes efficiency, integration, and evidence-based programming. The strategy commits to "streamlined foreign assistance" and "results-driven partnerships" with other governments, and it highlights PEPFAR's "robust data reporting and monitoring systems" as a model for accountability. The data blackout makes it difficult to verify whether the State Department is applying its own principles. Without historical data, it is also impossible for anyone outside the State Department to assess what the U.S. contribution to those decades of progress actually was, or to verify that current planning is informed by that baseline. And without fiscal year 2025 data, there is no way to independently determine whether the transition maintained that contribution or whether backsliding has occurred that requires recovery efforts.
Historical data matters immediately for the bilateral agreements now being negotiated. To date, the U.S. government has signed 31 bilateral health memoranda of understanding with partner countries. The implementation planning process—which was set to run through March 31, 2026, and is now delayed—required countries to develop strategies for each health area and to provide "data outlining the rationale for prioritizing the strategy" for each approach they propose. Countries were also set to establish targets for specific process metrics, including numbers of new HIV diagnoses, people on antiretroviral treatment, facility deliveries, and children receiving nutrition interventions, that will be used to track performance over the five-year agreement period. However, a recent Amfar report suggests that—in addition to use of flawed metrics—confidentiality agreements all but guarantee that although the U.S. government and countries themselves will have access to data, the public likely will not.
Without baseline comparison data, there will be no way to evaluate whether the new bilateral approach is producing better or worse results than prior aid-centric strategies, making it impossible to determine whether the transition represented improvement, continuity, or decline. Without a shared evidence base, there is no way to verify that implementation planning is truly evidence-driven, undermining both the collaborative approach and the data-informed decision-making that the State Department's own strategy emphasizes.
Transparency in Practice
If the United States is truly committed to efficiency, integration, and impact, restoring transparency would require three concrete steps.
First, although the new tool provides access to select global health data, the State Department should archive full historical PPR data, across sectors, on an official government website such as foreignassistance.gov or data.gov.
Second, the United States should publish any available data from fiscal year 2024 and 2025—with appropriate caveats about data quality and collection limitations—which would be far more valuable than releasing nothing at all.
Finally, the State Department should recommit to publicly publishing annual results for countries with bilateral agreements, including a core set of indicators tracking maternal and child health service coverage, HIV treatment and prevention continuity, malaria and TB service-delivery trends, and health facility functionality moving forward.