Acute malnutrition, a life-threatening condition characterized by sudden and severe weight loss, is a leading cause of death among children globally. If left untreated, more than 50% of children with severe acute malnutrition die, but with proper care this number falls to below 5%.
In many cases, treatment is simple and inexpensive. It costs between $100 and $200 to provide a full treatment of specially formulated foods such as Plumpy'Nut peanut paste to a child facing severe acute malnutrition. The availability of cost-effective treatment has driven substantial investment into programs to address acute malnutrition globally. Between 2017 and 2022, funding for these programs increased from $347 million to $591 million.
This progress hit a roadblock during the first 100 days of the Donald Trump administration when officials largely dismantled the U.S. Agency for International Development (USAID), firing or placing on leave nearly all staff, canceling about 90% of international development grants and contracts, and transferring remaining operations to the State Department.
USAID has historically funded large amounts of humanitarian food assistance. In the turmoil of USAID's dismantling, contracts with the World Food Program and other groups delivering emergency food assistance have been paused or canceled and reinstated repeatedly. Administration officials have stated that "essential lifesaving programs" would continue, but repeated disruptions have challenged their stability. European Union countries and the United Kingdom have also announced planned reductions in their foreign aid budgets. As a result of these cuts, the World Food Program faces a substantial budget shortfall of $11.35 billion in 2024. A recent analysis estimated a possible global reduction in treatment for severe acute malnutrition funding of 49% in 2025, approximately $290 million.
To evaluate the potential impact of increases and decreases in services to prevent and treat malnutrition in children, our team developed a computer simulation that illustrates the relative impact of alternative packages of antenatal and child nutrition interventions as well as their costs. This model can search for the best combination of interventions within a fixed budget, and the findings reinforce the importance of treatment for severe malnutrition.
The computer model runs by simulating a population of individuals who can experience malnutrition, disease, or death based on the risks seen in their local area in Nigeria, as informed by the 2021 Global Burden of Disease study. In Nigeria, which is home to the greatest annual number of deaths attributable to child malnutrition of any country, current programs to treat acute malnutrition save an estimated 39,000 child lives annually. However, existing programs fall well short of meeting need.
How Children Experience Malnutrition and Treatment
Without treatment, individuals are more likely to die from severe wasting

With treatment
Healthy
Measles
Wasting treatment
Malnourishment
Mild wasting
Moderate wasting
Severe wasting
Birth
5 years of age
Without treatment
Healthy
Measles
Malnourishment
Mild wasting
Moderate wasting
Child dies
Severe wasting
Birth
5 years of age
The chart shows how individuals experience malnutrition, disease, and sometimes death based on treatment in IHME's simulation.
Chart:
Adapted from IHME by CFR/Allison Krugman
•
Source
:
IHME

With treatment
Healthy
Malnourishment
Wasting
treatment
Measles
Mild wasting
Moderate wasting
Severe wasting
Birth
5 years of age
Without treatment
Healthy
Malnourishment
Measles
Mild wasting
Moderate wasting
Child dies
Severe wasting
Birth
5 years of age
The chart shows how individuals experience malnutrition, disease,
and sometimes death based on treatment in IHME's simulation.
Chart: Adapted from IHME by CFR/
Allison Krugman • Source: IHME
The model shows how the total figure for malnutrition, disease, and death varies across a population in response to different levels of available services and treatments. Because these conditional projections use 2021 data, estimates could be different than reasonably anticipated for 2025.
This model has generated an interactive tool that can help explore the impact of alternative nutrition interventions and the optimal way to allocate funds to achieve the largest improvement to child health. In the face of current funding instability, this model and tool could be used by decision-makers in the United States and Nigeria seeking to understand funding choices and their impacts.
Slashing Nutrition Treatment Could Lead to Excess Deaths
In Nigeria, funding cuts could lead to almost 19,000 additional child deaths from malnutrition

Baseline
Additional deaths with 49% reduction
The chart shows baseline and new excess deaths expected from malnutrition in Nigeria if funding is cut by 49% as projected by IHME's
computer simulation. Each child in the image represents approximately 483 deaths from malnutrition in Nigeria.
Chart:
Adapted from IHME by CFR/Allison Krugman • Source: IHME

Baseline
Additional deaths with 49% reduction
The chart shows baseline and new excess deaths
expected from malnutrition in Nigeria if funding is cut by
49% as projected by IHME's computer simulation. Each
child in the image represents approximately 483 deaths
from malnutrition in Nigeria.
Chart: Adapted from IHME by
CFR/Allison Krugman
Source: IHME
Although increased investment in acute malnutrition treatment could achieve further reductions in child mortality, recent threats to funding for these programs could lead to a reversal in course. Even modest reductions in services could result in additional thousands of children's lives lost. In the face of such threats to services to address malnutrition, it is worth evaluating what is at stake.
What the Nutrition Simulation Found for Nigeria
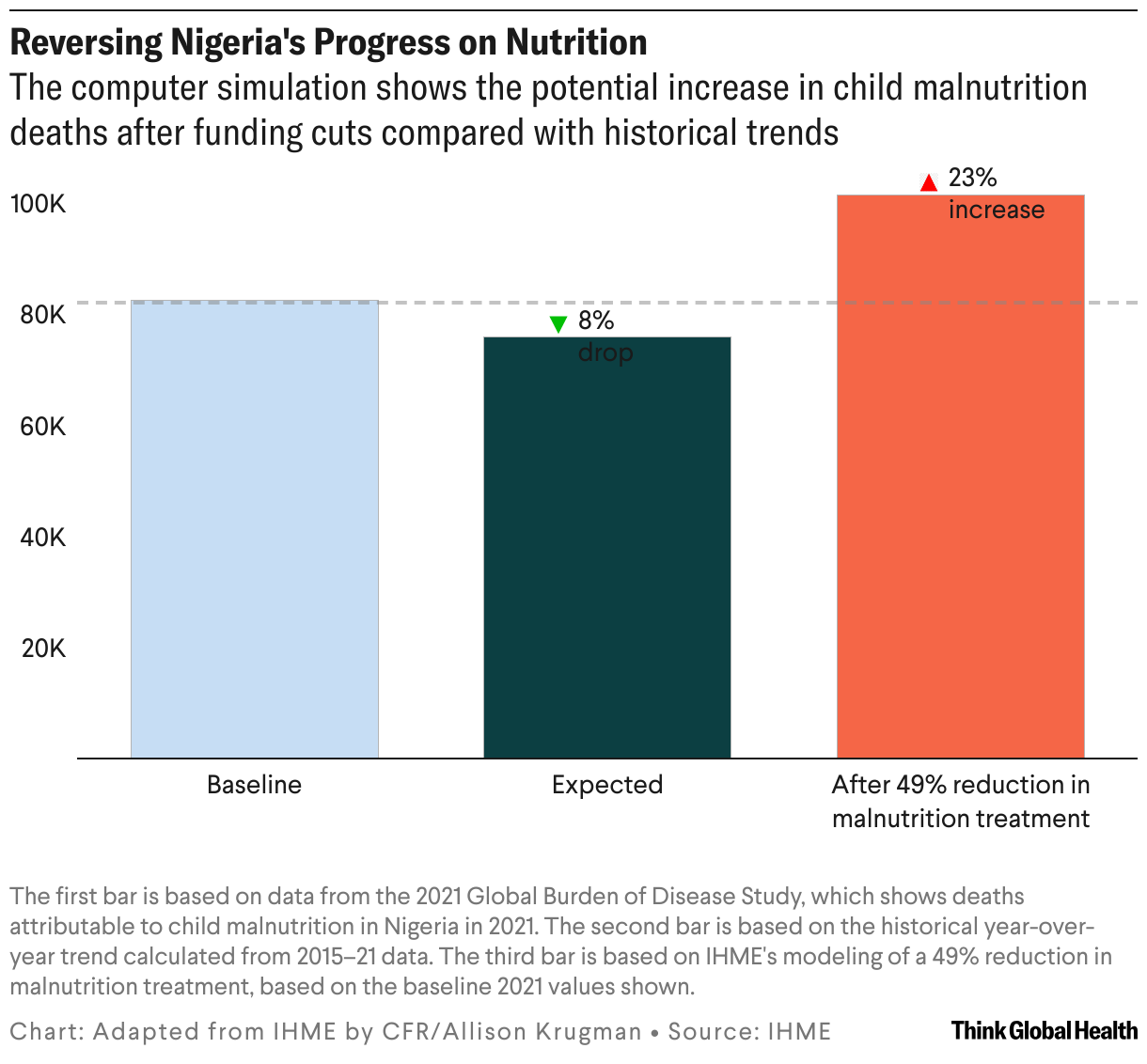
The analysis focused on a handful of locations, including Nigeria. The simulation shows that a 49% reduction in treatment of malnutrition in Nigeria would result in an additional 19,000 annual child deaths, a 23% increase from what would be expected otherwise.
Although the simulation used an estimated 49% reduction, uncertainty about the future funding of malnutrition treatment is considerable. To better understand the range of possible mortality anticipated, we also simulated a 25% and 75% reduction in funding. These scenarios resulted in 9,800 and 29,000 additional child malnutrition deaths from baseline, respectively.
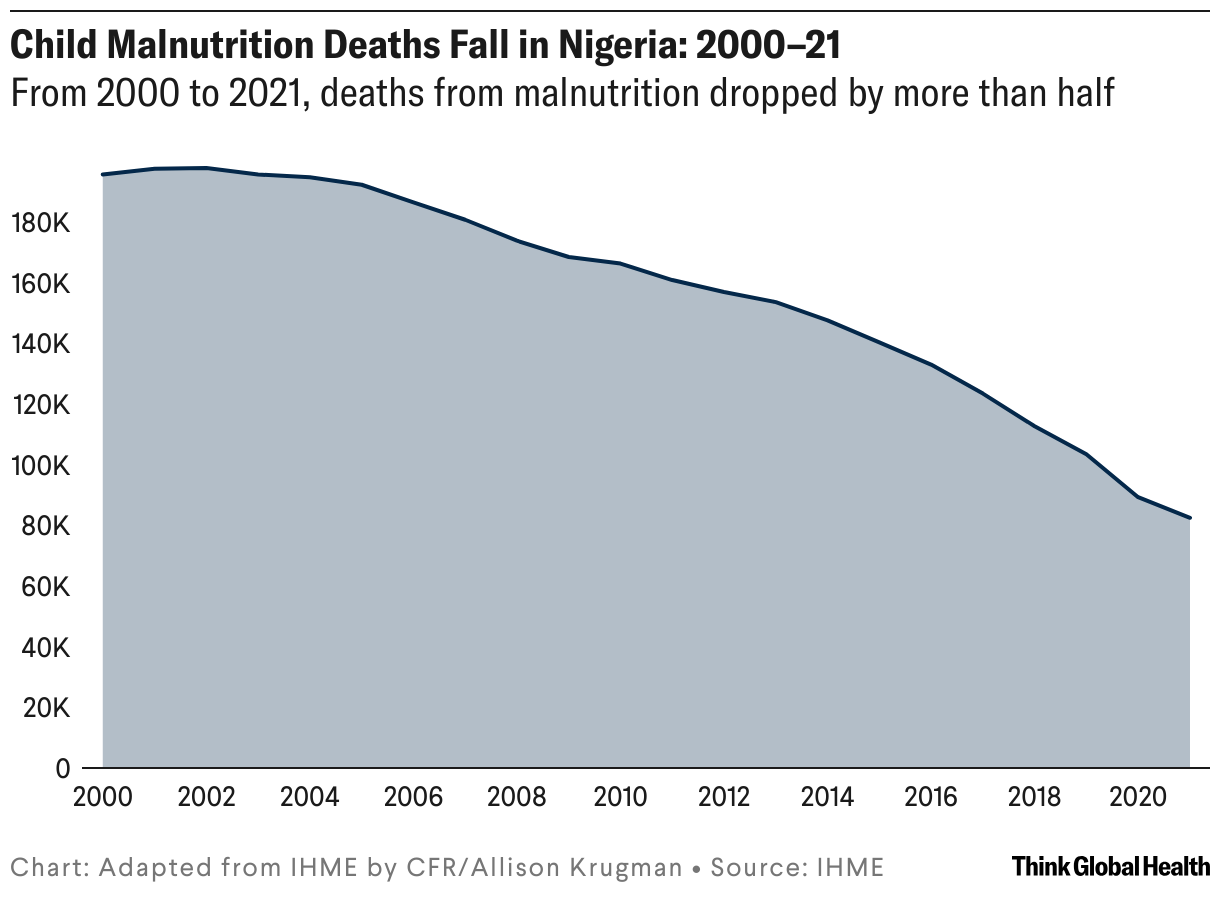
This finding highlights that even a more modest reduction in funding would lead to almost 10,000 young lives being lost. The increase in child fatalities estimated as a result of such treatment reductions would be a stark reversal of the consistent drop in child malnutrition deaths observed over the past 20 years in Nigeria.
These values could be underestimates of total impact on malnutrition mortality because cuts to other areas of the health sector could indirectly exacerbate malnutrition burden given ripple effects not included in the simulation. Without vaccine programs, more children will get infectious diseases; repeated bouts of infections, or certain conditions such as tuberculosis (TB), could then lead to increases in malnutrition.
On the Front Lines of Malnutrition and Foreign Aid Cuts
Vivianne Ihekweazu, managing director of Nigeria Health Watch, says that support for USAID and other donor groups has been critical to Nigeria's health system. "USAID's programs are deeply integrated into service delivery at federal and subnational levels," Ihekweazu said via email. "Unfortunately, we are going to see the collateral impact of the abrupt pull out of funding that has not left enough time to make plans for alternative sources for many of the programs that will be adversely impacted."
Although international support has saved lives, Ihekweazu also told us that Nigeria's reliance on external funding sources "has put the country in a very precarious position that no one was at all prepared for or even expected." She notes that Nigeria's "public health response has become heavily reliant on vertically funded programs such as those for HIV, TB, malaria, and polio often operating in silos and leading to inefficient health-care delivery. [Although] these vertical programs achieved specific disease control milestones, they also created fragmentation in Nigeria's health system. This fragmented approach hindered an integrated and coordinated response during the COVID-19 pandemic and continues to pose challenges in aligning resources effectively."
The Africa Centres for Disease Control and Prevention (Africa CDC) has detailed a plan to respond to declining official development assistance that includes a call for increased domestic public health funding from African Union member states. According to Ihekweazu, however, contributions from the Nigerian government "have historically been inadequate, with health spending hovering around 5% of the national budget—well below the 15% Abuja Declaration [PDF] target." She states that "political will is important now more than ever and the current government needs to demonstrate that they are able to forge a pathway to self-reliance for the country."
"For many years there has been advocacy for domestic resource mobilization for our health sector, and we hope this will be a moment that will be seized that will redefine how our health sector is funded," she continues. However, she cautions that although "the transition from vertical programs to integrated service delivery [is] necessary for sustainability, [it] is time and capacity intensive. [Because] donor funding is being pulled before the system is fully ready, Nigeria risks losing the hard-won gains made in disease control."

AUTHOR'S NOTE: All statements and views expressed in this article are solely those of the individual authors and are not necessarily shared by their institution.