As November begins, the U.S. government shutdown shows few signs of a resolution, as fierce disagreements continue over health-care spending.
The budget impasse centers around enhanced subsidies introduced under the Affordable Care Act (ACA), which are due to expire at year's end, making coverage even more expensive and inaccessible for low-income families. Democrats refuse to back to a continuing budget resolution without health-care guarantees in part because the One Big Beautiful Bill Act (OBBBA), signed into law in July 2025 by Republican President Donald Trump, reduces federal Medicaid spending by $911 billion and could increase the number of uninsured by 10 million people over the next 10 years.
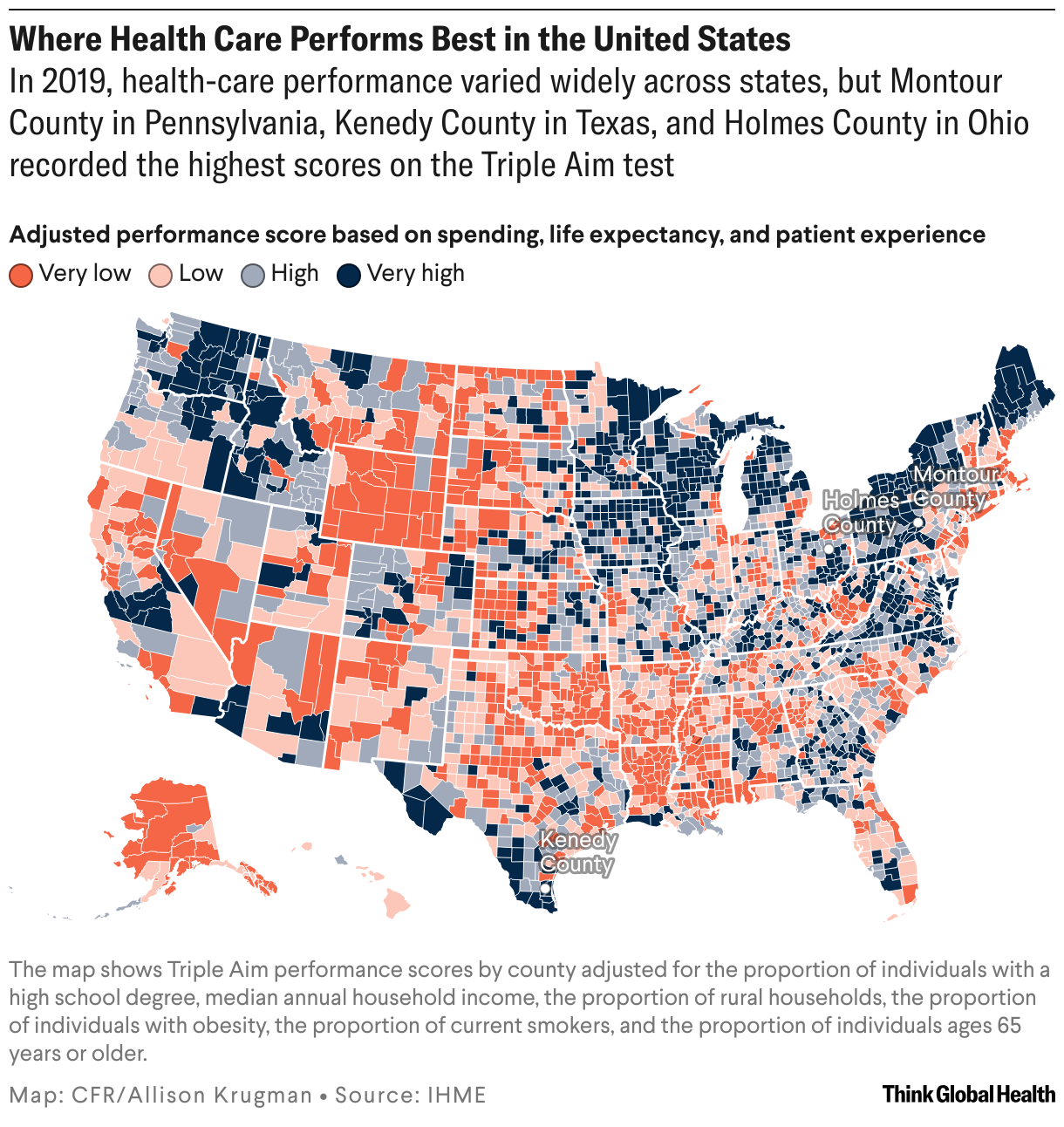
A new study from the Institute for Health Metrics and Evaluation (IHME) underscores the pitfalls of cutting federal insurance programs, that expanded Medicaid coverage was associated with higher scores on the Triple Aim test—a metric that rewards positive patient experience, stronger health outcomes, and lower health-care spending per capita. This finding held firm after adjusting for characteristics such as wealth, education, obesity, and smoking. The study indicates that although health disparities persist between states and counties, evidence-based design can still deliver high quality care and improve outcomes relative to a county's demographics.
"More than 85% of the counties in Idaho, Iowa, Maine, Washington, and Wisconsin all had positive adjusted performance scores," said Haley Lescinsky, a managing research scientist at IHME and the lead author on the study. "Meaning that within these states, most of the counties are doing better than you would expect given the population characteristics."
IHME's findings indicate that to improve health-care performance, states and counties will need to challenge existing trends, including hospital and insurance consolidation and shrinking Medicaid coverage.
Measuring Health-Care Performance
Created in 2008, the Triple Aim framework gauges health-care performance along the dimensions of life expectancy, patient experience, and health spending. Governments have used this framework to evaluate system performance and guide decision-making in the United States, Canada, Ghana, and the Netherlands. The IHME study scores U.S. counties on their progress toward Triple Aim.
As a country, the United States performs poorly. Health-care spending was nearly 17% of U.S. GDP in 2023, or more than $13,000 per capita. On average, comparable high-income countries spent about $7,000 per capita on health—roughly half the U.S. mark. Despite the high costs of care, the United States has the lowest life expectancy and poorest care experience among its peer countries.
Beyond the national level, however, variation between U.S. states and counties is widespread. IHME's study sought to measure those differences and identify which characteristics and policy levers drive them.
Consistent with other research on the social determinants of health, IHME found that high-scoring counties were generally wealthier and more educated, and had lower rates of obesity and smoking. They were also primarily urban.
"Income and education matter," said Joseph Dieleman, a professor who coauthored the study and leads IHME's health resource tracking team. "Essentially, privilege was associated with better performance."
At the county level, the picture was more nuanced: Washington, DC, for example, had better outcomes but high spending, leading to a lower overall score. Some rural counties in Texas and Ohio performed well despite their older and less healthy populations by delivering quality care at lower spending levels.
Policies Shaping Care
After controlling for system-level characteristics, researchers were able to pinpoint the policy factors that shaped better-performing systems.
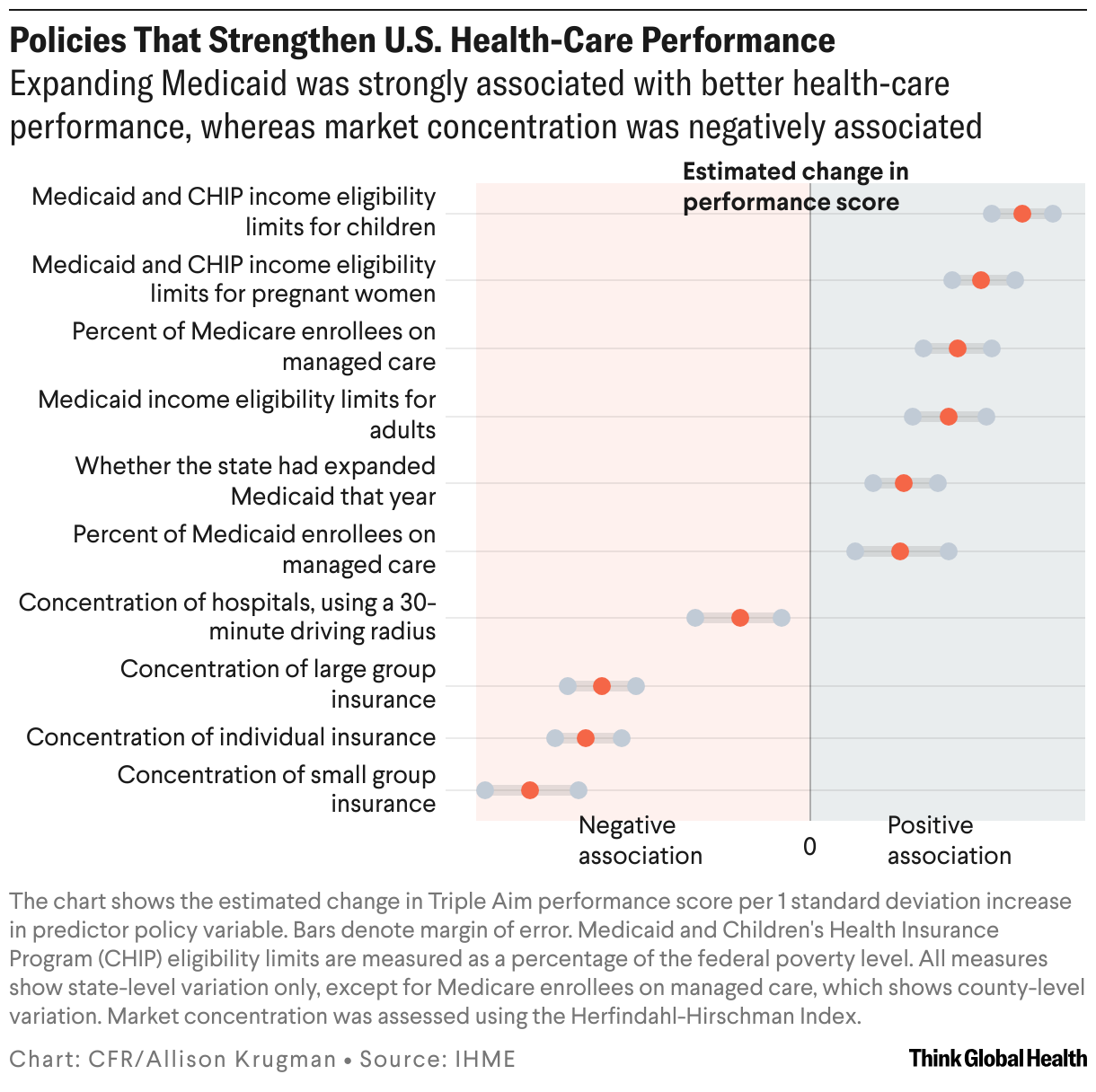
Consolidation has been increasing in the U.S. health-care market—when hospitals or insurers merge, or when private equity firms and other entities purchase medical practices. This trend has driven up health-care costs for patients and federal programs. According to the U.S. Government Accountability Office, nearly half of physician practices were consolidated with hospital systems in 2024, up from less than 30% in 2012. Market concentration varies across states, Alaska and Alabama having the highest levels in 2019 according to IHME. States such as Minnesota have begun to take action to halt consolidation through regulation and by considering public interest in evaluating mergers.
"Less competition in insurance and hospital markets can lead to higher spending and isn't associated with higher quality," said Dieleman. "We would highlight this as an opportunity for reducing costs within the health system."
Conversely, IHME identified Medicaid expansion as a valuable lever to reduce individual medical costs, improve quality of care, and increase life expectancy. The study period begins in 2014, the year the Affordable Care Act offered states the opportunity to expand Medicaid, and ends in 2019. The study found that expanded eligibility limits on Medicaid and Children's Health Insurance Program had the highest association with positive health-care performance.
Previous research [PDF] mirrors these findings, showing that states that chose to expand access to Medicaid under the ACA not only had better health outcomes, but also better educational outcomes for young enrollees, who also had higher earnings as adults.
Medicaid, jointly funded by states and the federal government, provides health insurance to low-income families, including children and the elderly, people who are pregnant, and people with disabilities in the United States. The 41 states that chose to expand Medicaid under the ACA offer coverage to a greater number of adults: those making up to 138% of the federal poverty level, or $21,597 for an individual, in 2025.
"[States that expanded Medicaid] had higher levels of performance," said Dieleman. "That is an important takeaway, and it suggests that there could be some very serious repercussions from removing Medicaid or disenrolling lots of individuals from Medicaid."
Challenges Ahead for States and Counties
The OBBBA cuts will largely affect those benefiting from expanded Medicaid, including young people who otherwise would not have qualified based on income alone. Those populations are set to face higher out-of-pocket costs and limited access to care.
In one measure currently being challenged in the federal district court of Massachusetts, the OBBBA prohibits Medicaid funding from some providers offering reproductive health care or family planning, which will disproportionately affect young women.
"Achieving the Triple Aim is not about just achieving low spending to the detriment of the people in the health system," said Dieleman. "It requires a nuanced policy perspective in both service delivery and health system design."
Major changes to the U.S. health system at the federal level could force states to develop creative approaches to meet the needs of their populations, such as leveraging emergency reserves or tobacco taxes to serve low-income populations.