
Between 2000 and 2010, the field of global health underwent a revolution that redefined development assistance, reshaped international institutions, and created relationships of dependence among nation states. It happened during a period of optimism fueled by a mix of scientific understanding, compassion, and expansive global ambition—a period quite different than today. The current challenge for global health is adapting institutions and approaches built for growth, speed, and external intervention for a very different future.
Let's start with how it used to be. For many years before the turn of the millennium, the field that we now call global health—then labeled "international health" (and, earlier, "tropical medicine")—existed in a stable equilibrium. The field was the purview of a small number of organizations, with total funding from official development assistance of less than $10 billion per year, of which about one-third came from the United States government. A handful of universities, including Johns Hopkins, Tulane, and the London School of Hygiene and Tropical Medicine, trained international health professionals at the graduate level, and most were physicians with a taste for adventure. The Rockefeller Foundation and a few other private foundations in the United States invested in these institutions, as well as in building research and implementation capacity in Latin America, Asia, and Africa.
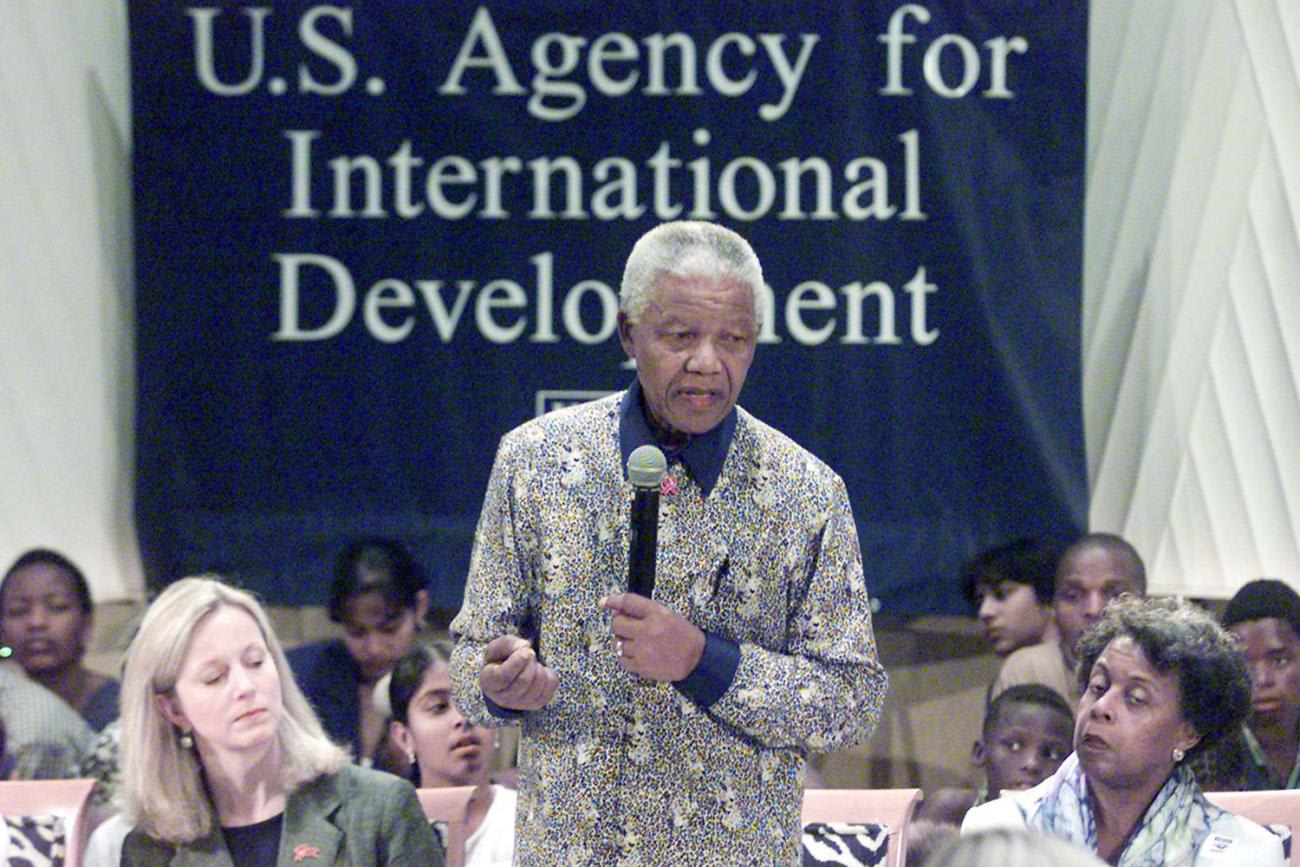
A handful of universities trained graduate professionals—mostly physicians with a taste for adventure
Within the U.S. Government, programs were largely delivered through the U.S. Agency for International Development (USAID), which focused since its inception in the mid-1960s on family planning, maternal and child health, and a few tropical infectious diseases. The majority of funding went through a small number of grantees and contractors. Separately, the Centers for Disease Control and Prevention had a modest unit working internationally, primarily in support of smallpox eradication and other targeted programs at the World Health Organization. In addition, the Department of Defense dedicated resources to research on diseases of particular importance to the military, including malaria.
On the multilateral front, in addition to obtaining technical support from the World Health Organization, low- and middle-income countries could borrow from the World Bank and regional development banks for health infrastructure, health worker training, and system reform. UNICEF designed and implemented child health programs organized around low-cost interventions: growth monitoring, oral rehydration, breastfeeding, and immunization with off-patent vaccines that could be purchased for pennies a dose. Industry was not at the table and, in fact, was largely reviled for its approach to maximizing profits and, in the case of baby formula manufacturers, predatory marketing.
Kicking Into High Gear
A series of disruptions dramatically shifted the narrative, funding, and players in ways that set the stage for what we have today. Only an historian could fully describe and explain the forces that came together in the early part of the century, but here's a high-level overview of three of them: the Millennium Development Goals, the Bill & Melinda Gates Foundation, and the response to the AIDS pandemic. Together, these factors pushed and pulled the field into a phase of unprecedented growth in ambition and scale.
Of the eight Millennium Development Goals established in the year 2000 by 189 UN member states, three were directly related to health: reducing childhood mortality, improving maternal health, and combatting HIV and malaria. Countries committed to making faster progress toward these goals than had ever been seen in recorded history. While the lack of realism was apparent, the existence of the goals forced conversations within UN agencies and aid agencies about how much more funding and political support would be needed to accelerate gains. In a radical departure from the earlier question of how many lives could be saved with the resources available—what the cheapest life-saving interventions were—advocacy attention turned toward demanding resources sufficient to achieve the goals.
That same year, the Bill & Melinda Gates Foundation was established. If the Millennium Development Goals sparked the imagination about what might be possible, the emergence of the Gates Foundation—promising significant new spending and incisive, businesslike thinking—lit the fire. One of the foundation's earliest initiatives was an investment of $750 million to start the Global Alliance for Vaccines and Immunization (GAVI) and its funding arm, the Vaccine Fund (now the Vaccine Alliance). Along with the new money for childhood immunization came a strikingly new narrative: that GAVI would work with partner countries, UN agencies, and (gasp!) the pharmaceutical industry to accelerate access in low-income countries to the newer vaccines that were available in the United States and other wealthy countries. Children in poor countries would not only be getting inexpensive, off-patent traditional vaccines; they would, with financial and technical support from outside, get an on-patent five-in-one shot that included vaccines for hepatitis B, Haemophilus influenzae type b, diphtheria, tetanus, and whooping cough. Moreover, GAVI was expected to accelerate introduction of other life-saving vaccines as they obtained regulatory approval.
Between its work on vaccines and its other programs, the Gates Foundation was soon spending around $1 billion a year on global health—close to the total USAID global health budget at the time. The surge in resources, and the attention by a famous person to the unglamorous cause of poor people's health, attracted many existing and new NGOs, and motivated a large number of U.S. universities to establish cross-disciplinary global health programs.

The sense of ambition stemming from the the Millennium Development Goals and the early work of the Gates Foundation paled alongside the global response to AIDS. While the world came too slowly to recognize the importance of fighting HIV/AIDS, a sea change finally occurred. By the year 2000, more than 25 million people in sub-Saharan Africa were infected with HIV, and some four million were newly infected each year. The disease struck down millions of people in the prime of their lives, devastated whole communities, and reversed hard-won gains in life expectancy in many countries. Yet unlike many of the "tropical diseases" and public health problems that had been the focus of global health to that point, HIV/AIDS was a domestic concern in the United States and Europe, where the disease was also hitting hard. Activists in wealthy countries, many of whom were themselves living with HIV/AIDS, aggressively lobbied for newly developed antiretroviral therapies to be made available not only within their own communities but also to those suffering from the same disease elsewhere.
Their efforts have forever changed the nature of health advocacy. More than any other health cause before, advocates brought passion, political savvy, and powerful tactics to bear on donor governments and pharmaceutical manufacturers: make the expensive drugs available, scale up life-extending treatment as quickly as possible, and focus on HIV/AIDS as an existential threat. (The recent Forbes article, "AIDS Activism, A Playbook for Global Health Advocacy," highlights many of the main tactics.)
Pushed and prodded, shamed and coaxed, the global community woke up to the challenge of HIV/AIDS. The Joint United Nations Programme on HIV/AIDS (UNAIDS) had been created in 1996 as a means to coordinate the UN response, but donors—finally feeling a sense of urgency—became frustrated with what was perceived as the slow-moving bureaucracy of the existing multilateral organizations. To mobilize and move money fast, they established the Global Fund to Fight AIDS, Tuberculosis, and Malaria in 2002. With a focus on scaling up access to antiretroviral treatment, the Global Fund collected and distributed large amounts of new resources from the U.S. and European governments—as well as from private contributors.
Pushed and prodded, shamed and coaxed, the global community woke up to the challenge of HIV/AIDS.
While contributing to the multilateral effort that had been negotiated on the global stage, the United States had more enthusiasm for a home-grown idea. The George W. Bush Administration worked with Congress to create the single largest global health program ever, the President's Emergency Plan for AIDS Relief. With an initial funding level of $15 billion and an organizational home separate from USAID, PEPFAR quickly became the dominant global health funder, channeling resources through a large number of U.S.-based NGOs and universities—many of them new to global health—and through U.S. government agencies taking on greatly expanded or entirely new international roles. The new money—the vast majority of it allocated to putting patients on antiretroviral drugs—attracted groups that had previously worked on family planning and maternal health. They pivoted to AIDS prevention and treatment. Other organizations that had expertise in health systems, health worker training, economic development, and education also did all they could to connect their work to the free-flowing AIDS money.
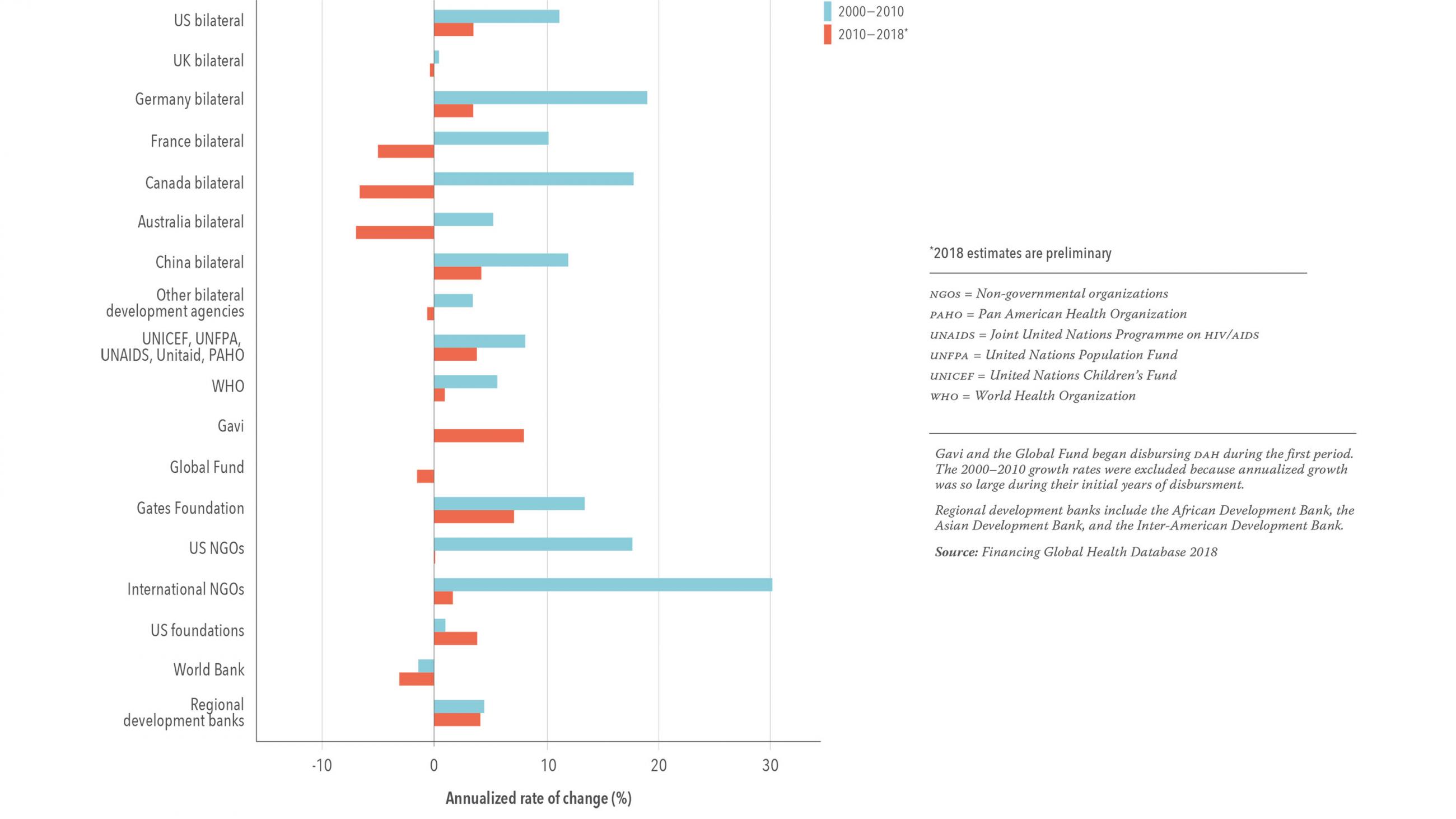
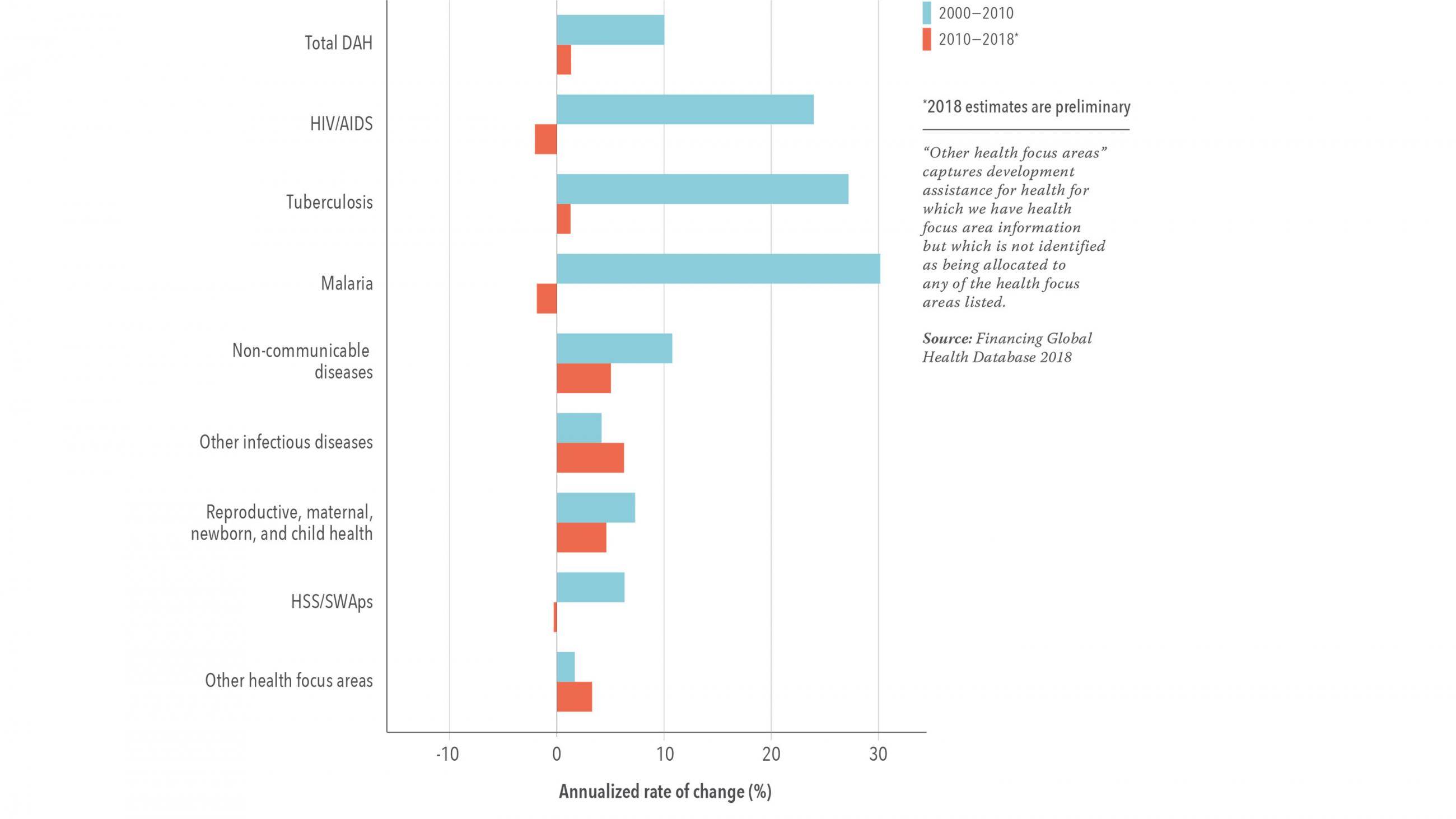
With PEPFAR the largest share of a growing pie, between 2000 and 2010, development assistance for health increased from about $12 billion to close to $40 billion. In addition to the emergence of GAVI and the Global Fund as major channels through which assistance flowed, the amount channeled through NGOs also increased. Many were recipients of PEPFAR dollars or received support under the U.S. President's Malaria Initiative, launched in 2005. In addition, a series of "innovative financing mechanisms," from the Advance Market Commitment for vaccines to the International Financing Facility for Immunization to Unitaid to the Affordable Medicines for Malaria initiative, were designed, resourced with billions, and launched in the capital cities of the largest donors.
Along with the money came results that could be expressed not only in drugs and vaccines delivered and bednets distributed, but in human lives saved. GAVI has helped to immunize more than 760 million children, preventing an estimated 13 million deaths. PEPFAR reports that it supports more than 15 million people with antiretroviral medications in 50 countries, The Global Fund estimates that the AIDS, TB, and malaria programs it supports have saved a total of 32 million lives. For its part, the President's Malaria Initiative says it has saved 7 million lives.
That short summary does not do justice to the amount of commitment and creativity that characterized global health during the early part of the century, but it gives a sense of the period of rapid expansion in which a small number of health priorities, interventions, and funding sources dominated. Along with the resources and technical expertise, these priorities came from outside of the countries receiving the aid, as did the expectations about how fast new drugs and vaccines would be integrated into existing health systems. The models of engagement with national governments and of service delivery were built for speed, not long-term affordability, and the pace left little time for deliberating about the most sustainable path or doing the painstaking work of building systems along with delivering services.
The pooled funds, parallel delivery systems, and externally defined priorities created a complex and fragmented architecture at the international level, and massive challenges for governments being asked to welcome help regardless of the ability of countries to take over either funding or operations over time. The influx of funds and imperative to use them for fast results led to an expansion of international NGOs' engagement in health, with relatively little attention to efficiency, affordability, and long-term commitment. When financial and organizational sustainability was in tension with getting vaccines and drugs to those who needed them, sustainability took a back seat.
Stuck in High Gear, But No New Fuel in the Tank
Over the past decade, things have changed—in a big way. There have been almost no new resources for global health, and the considerable advocacy muscle of the global health community has had to focus simply on maintaining the current levels of bilateral and private commitments to support both longtime and newer initiatives. The U.S. government, still the largest global health funder by far, resists taking a leadership role as questions about the role of the United States in solving problems outside its borders have become caught up in the political maelstrom. Ditto for the UK government. The competition among agencies and interest groups has made coordination yet more difficult. And many of the young professionals coming out of undergraduate and graduate training programs in global health are finding that their hoped-for jobs simply aren't there.
More importantly, the global health community is recognizing that the battle for better health in poor countries will not be won disease-by-disease, vaccine-by-vaccine. And it won't be won by well-intentioned outsiders.
the battle for better health in poor countries will not be won disease-by-disease, vaccine-by-vaccine
Programs established to deal with particular diseases in particular ways are now being asked to align with host government priorities and improve systems. The delivery channels, procurement systems, and monitoring data that were created for a single purpose, once imagined to be time-limited, are now being asked to serve broader health systems long into the future. HIV/AIDS drug treatment programs are being touted as the potential starting point for much needed systems to deliver care to people with diabetes, hypertension, and other chronic conditions. Highly medicalized, patient-centered interventions are reorienting toward behavioral and social issues far outside their original remit. PEPFAR, for instance, now supports USAID's work addressing the structural inequalities that impact girls' vulnerability to HIV. In other words, the past ten years have been a period of adjustment to a new world—but with no new money to support the transition.
An Agenda for the Future
The global health community rose, in remarkable ways, to the challenges and opportunities between 2000 and 2010. Since then, it has been modifying agencies' original designs in piecemeal ways to meet entirely new challenges. But it cannot jury-rig its way to the future. There is a job to do, and it's one that requires fresh thinking
We need to take a hard look at the roles, responsibilities, and funding levels of different parts of the global health ecosystem.
We need to take a hard look at the current architecture—the roles, responsibilities, and funding levels of different parts of the global health ecosystem—and figure out which parts have a permanent role and which ones should be gracefully phased out. We have to create governance structures that suit a moment of geopolitical flux. We have to think through how the funds now available can be best used to achieve the greatest health gains—not only in particular disease areas, but across all health conditions. And, most importantly, we have to find ways to work with low-income countries that have been dependent on development assistance for health so that they strengthen their own health systems and mobilize resources through effective taxation.
In many ways, this is as exciting and inspiring an agenda as the rush to distribute life-saving drugs, but it will require different skills and different ways of working. I, for one, am hoping that's precisely what the new generation of global health professionals has.











