In defending against a potential influenza pandemic, Vietnam has responded impressively. During the 2005 outbreak of H5N1 avian influenza, it rapidly diagnosed and shared data on H5N1 infections and vaccinated and culled poultry to slow the outbreak. Those actions contributed to global efforts to thwart the emergence and spread of dangerous influenza viruses. Vietnam deepened its commitment to countering influenza threats by moving toward producing its own vaccines.
Vietnam's success partly lies in the Global Action Plan for Influenza Vaccines (GAP), a World Health Organization (WHO) initiative launched in 2006 that boosted Vietnam's capacity to make influenza vaccines locally. The world would be wise to build on such projects as efforts to expand vaccine production in developing countries get under way after the COVID-19 pandemic.
The Global Action Plan
The WHO created the GAP in response to the rapid, worldwide spread of H5N1 avian influenza. The specter of a potential pandemic revealed a glaring vulnerability: less than 2% of the world's influenza vaccine supply would reach low- and middle-income countries quickly during a crisis. Back then, more than 90% of influenza vaccine production was done in only nine countries, mostly in Europe and North America, that represented only 10% of the global population. That disparity rendered people in countries across Africa, Asia, and the Middle East vulnerable because, in an emergency, countries with local production would likely prioritize their own populations before distributing to others. Recognizing a need to address that collective risk, the WHO announced the GAP, which continued through 2016.
Less than 2% of the world's influenza vaccine supply would reach low- and middle-income countries quickly during a crisis
The GAP's chief aim was to boost vaccine production capability across the developing world so that more countries could protect populations against threats emerging locally that could spark global crises. The plan also promoted seasonal influenza vaccine programs that drive vaccine demand and support research on new vaccines.
To meet the production pillar, the WHO selected 15 countries that were not making pandemic influenza vaccines but could, including Brazil, China, Egypt, India, Indonesia, Romania, Serbia, Thailand, South Africa, and Vietnam. At launch, the GAP had $10 million, but a $98 million commitment from the U.S. Biomedical Advanced Research and Development Authority (BARDA) drove donors and other countries—particularly those receiving GAP assistance—to commit additional funds. By 2016, such countries had invested an average of $17 for every dollar spent by BARDA.
When the GAP ended in 2016, participating countries had the cumulative capacity to produce 1.3 billion doses of pandemic influenza vaccines annually as needed for pandemic response—potentially amounting to 20% of the global emergency supply. When not making pandemic vaccines, those countries produced vaccines against seasonal influenza. The world went from having the capacity to produce 350 million doses of seasonal influenza vaccine in 2006 to the ability to make more than 1.47 billion doses in 2016. Pandemic influenza vaccine production capacity increased from approximately 1.46 billion to 6.37 billion doses.

Influenza Vaccines from Scratch
Vietnam showcases the potential of vaccine-production initiatives. When the GAP launched in 2006, Vietnam appeared disadvantaged relative to other GAP-supported countries because it had one of the smallest economies and no influenza vaccine production. However, Vietnam's repeated experiences with avian influenza—and delays of nearly a year in securing vaccines from other countries during the 2009 H1N1 influenza pandemic—highlighted a dire need for self-sufficiency. In addition, expensive imported vaccines were not always effective against the viruses circulating in the region.
Vietnam's manufacturing company, the Institute of Vaccines and Medical Biologicals (IVAC), took longer to develop and obtain regulatory approval for vaccines than entities in other GAP-supported countries. IVAC's steady efforts culminated in the licensure in 2019 of its first domestically produced human seasonal influenza and pandemic influenza vaccines.
One barrier that Vietnam faced was the lack of a reliable source of vaccine-quality chicken eggs. After several years of attempting to import eggs from other countries, the government decided to build a new chicken facility to supply the vaccine factory. That decision eliminated a critical supply chain issue that an influenza outbreak could easily exacerbate.
National production reduced vaccine prices by nearly a third of the cost per dose, making influenza vaccination economically viable for a broader demographic. A 2020 report indicated that the willingness to pay for influenza vaccines among Vietnamese women aligns closely with costs. Further, nationally branded vaccines garnered trust.
Nationally branded vaccines garnered trust
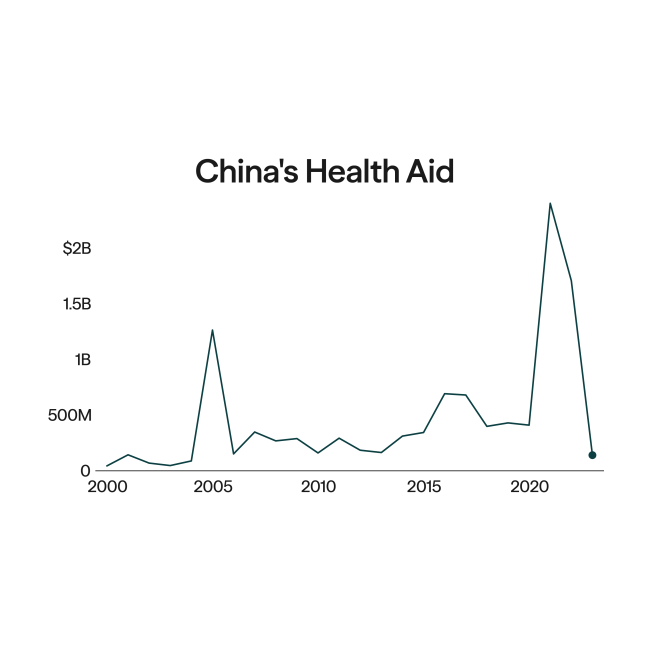
South Korea, a high-income country with a decent biotechnology sector, was, unsurprisingly, the first GAP-supported country to have locally made pandemic influenza vaccines approved. As a result, it quickly developed and produced vaccines to protect the country during the 2009 H1N1 pandemic. Economic status, however, was not the main predictor of success. For example, Brazil, China, India, and Thailand became seasonal and pandemic influenza vaccine producers through the GAP, whereas Romania, a high-income country, continues to rely on imports.
Instead, government prioritization, sustained financial support, and the uptake of seasonal influenza vaccines mattered most. After all, manufacturers cannot survive without an adequate marketplace for their products. That issue might have contributed to halting South Africa's GAP-supported program at the government-run facility, Biovac. In one study in South Africa, only about a quarter of health-care workers, who are at high risk of severe influenza, opted to take seasonal influenza vaccines.
Influenza vaccine production in Indonesia, Kazakhstan, and Romania also failed to flourish after the GAP ended. Those countries succeeded in producing authorized, domestic influenza vaccines but continue to import most of what they need because their national facilities cannot make enough doses. Indonesia imports vaccine components and formulates them into final vials. Romania closed its original facility but plans to open a new one in 2025.

Pandemic Preparedness
Beyond scaling up influenza vaccine production, the GAP sought to empower countries to develop the scientific foundation needed to curb local outbreaks rapidly. During the GAP's existence, more than 300 manufacturing and regulatory experts trained on advanced biomanufacturing and quality systems at two facilities in the United States. Vaccine production experts from BARDA and PATH helped ensure that such training strengthened the operation of local facilities. Frequent workshops between GAP participants and leading vaccine experts around the world created a global network of colleagues that continues to share knowledge.
National regulatory capabilities grew as well. At the outset, only four GAP-supported countries had a functional national regulatory authority qualified by the WHO to evaluate clinical trials, license products, and conduct postmarketing surveillance. At the plan's conclusion, that number had grown to 10, and the remaining countries were on course to accomplish the milestone. By meeting the WHO's regulatory quality standards, countries have the opportunity to distribute their vaccines to other countries.
Another aspect of the GAP proved broadly beneficial. Global pandemic influenza vaccine capacity had been limited by a small number of companies holding patents for making ingredients—called adjuvants—that enhance vaccine efficacy and expand vaccine supply by reducing the main ingredients needed in each dose. The GAP helped fund the development of generic adjuvants at the Infectious Disease Research Institute and the University of Lausanne, an effort that led to the creation of the Vaccine Formulation Institute in Switzerland. By supplying the GAP's manufacturers, the institute nearly doubled the overall capacity of pandemic influenza vaccines produced by those companies.
Cracking the Egg for COVID-19 Vaccines
The foundation laid by the GAP became important during the COVID-19 pandemic when vaccines were again in short supply and many nonproducing countries were at the end of a long line for vaccines. GAP-supported companies in Brazil, Thailand, and Vietnam leveraged their systems for making egg-based influenza vaccines to produce those against COVID-19. Those facilities could be converted to make COVID-19 vaccines when not making seasonal influenza vaccines. Capacity in these three countries combined could yield hundreds of millions of doses per year. The GAP-supported Serum Institute in India played an outsized role in COVID-19 vaccine production and distribution nationally and globally.
Capacity in these three countries combined could yield hundreds of millions of doses per year
In addition, companies from the GAP network are collaborating with scientists at the Icahn School of Medicine at Mount Sinai in New York and the University of Texas at Austin to develop and evaluate a COVID-19 vaccine by using a modified Newcastle disease virus that grows in chicken eggs and produces the spike protein for the SARS-CoV-2 virus. Partnerships with PATH developed under the GAP program are also accelerating the production of a COVID-19 pandemic vaccine.
Local Solutions for Global Outbreaks
The GAP demonstrated the feasibility of expanding global vaccine production and empowering countries to respond to outbreaks. The plan helped unlock the immense latent value of local vaccine infrastructure when international supply chains fracture amid a public health crisis.
A more recent initiative launched in 2021, the WHO's mRNA technology transfer hub, seeks to replicate the GAP's success. Again, the WHO has selected 15 countries that would benefit from local vaccine production. The initiative focuses on a promising platform—mRNA—rather than a specific disease. Nonetheless, like the GAP nearly 20 years ago, the hub seeks to assist nations' quests for sustained agency, rather than persistent dependency, in the face of biological threats.

EDITOR'S NOTE: This article is part of a series on efforts to increase pharmaceutical production in developing countries guest-edited by Amy Maxmen. The other articles in the series can be found here.